Last week I came across this tweet posted by @GSKUS:
RT @NHF: Need help remembering your #migraines details? Find an online migraine diary from @GSKUS at http://bit.ly/hBS98Q
For my Twitter-challenged readers, I should point out that "RT" signifies that @GSKUS "retweeeted" a tweet originally made by @NHF, which is the Twitter account of the National Headache Foundation.
Whenever a pharma company retweets a message from a third party, it raises some flags. For example, suppose NHF was a patient advocacy organization that promoted off-label use of medications and suppose those medications were marketed by GSK? Further, what if GSK helps support NHF with funding? What if NHF received the majority of its funds from GSK? What if NHF was actually created by GSK and not independent at all?
These days there are quite a few tools I can use to answer my questions. But, first, let's look at the link in the tweet.
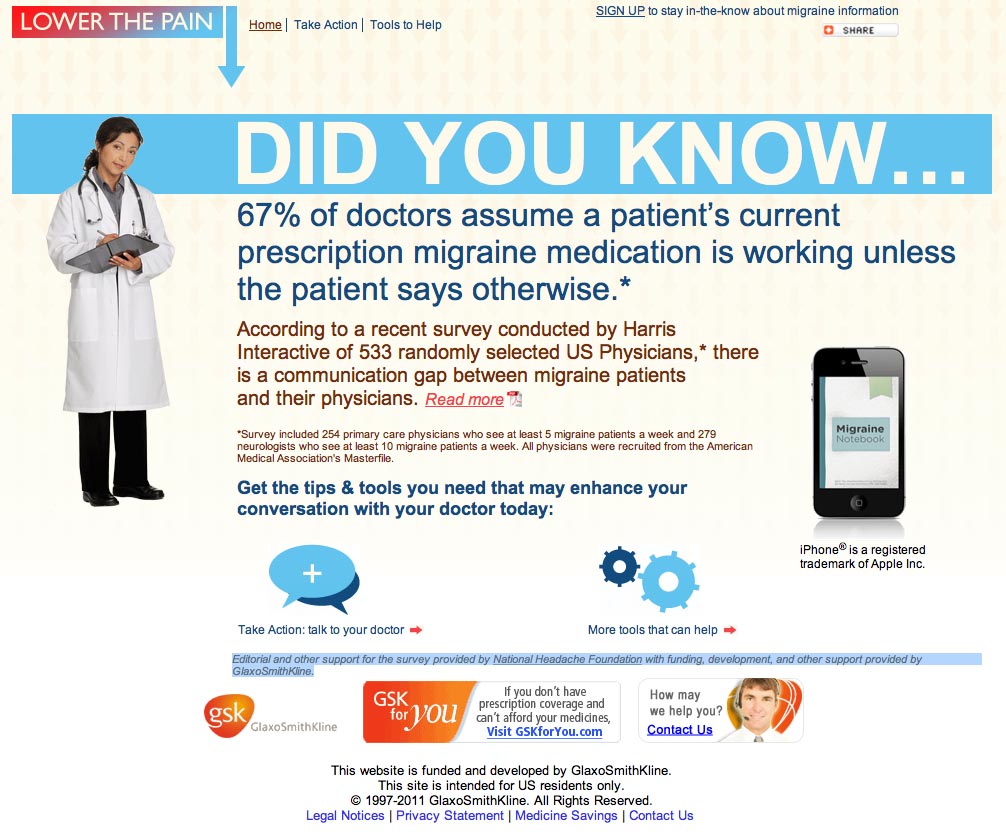
When you click on the http://bit.ly/hBS98Q link in the GSKUS tweet, you discover that the real link is http://www.lowerthepain.com/pdf/Migraine_Diary.pdf. The "Lower The Pain" website (www.lowerthepain.com) is a GSK site that prominently promotes a migraine survey. "Editorial and other support for the survey provided by National Headache Foundation with funding, development, and other support provided by GlaxoSmithKline," says GSK on the site. See this
Fact Sheet on the NHF site for more about the survey.
But I also see an invitation to get "tips & tools you need that may enhance your conversation with your doctor today." Right NEXT to that is a picture of an iPhone, which GSK is careful to point out is a registered trademark of Apple Inc.
When I click on "Tools to Help" I am brought to the following screen:
This further HINTS that there is an app for that (ie, "MIGRAINE DIARY").
So, is there an iPhone version of the Migraine Diary?
Yes, there IS an iPhone "Migraine Diary," BUT it does NOT appear to be a GSK app or an NHF app. Here's the app by that name that I found on iTunes:
This is a nice little app, but it does NOT resemble the GSK's PDF version of "Migraine Diary."
The iPhone app was developed by Net Workz LLC, a Software Engineering Firm located in the UK, which is the only connection I can see between it and GSK. In fact, the creator of the app is Aaron Douglas. His about page states that "Net Workz LLC is a small company I started that I use for anything I do geeky-related. I don’t have much content here but I plan on expanding this site soon. My full time job employs me as a software engineer. This place is for my personal projects that need to be legit, like iPhone Apps."
Maybe GSK and Douglas are negotiating a deal right now to allow "Migraine Diary" to "go legit."
The only comment Douglas has received about his app is this:
"I like this app. It's not the fanciest, but I wanted something easy to fill out when I'm in pain! The only problem I have is that sometimes when I add a journal entry, it only shows up when I turn it off then on again, but it is there. I wish it had more graphs to see more than one month, to see a patten. An option for an "all day" headache instead of having to put in a time would be good!"
OK, so what about the relationship between GSK and NHF? There's obviously the survey mentioned above. There's a guest post to GSK's blog by Merle L. Diamond, MD entitled "Teaming up to Close the Gap in Doctor-Patient Migraine Communication" (see
here). "Dr. Merle L. Diamond was compensated by GlaxoSmithKline for her participation in this campaign," GSK disclosed. Dr. Diamond is a member of the NHF board of directors.
Dr. Diamond is daughter to
Seymour Diamond M.D., Executive Chairman of NHF, who originally founded the National Migraine Foundation, which was renamed the National Headache Foundation in 1987.
Seymour Diamond is the also the founder of Diamond Headache Clinic and Merle Diamond is it's president.
I'm not going to track this much further, but it would be interesting to know how many other physicians involved with NHF and the Diamond Headache Clinic are on GSK's payroll. Now that GSK has been required to list all payments to physicians, it should be easy to find out.
OK, I will track this a bit further. I just downloaded NHF's 2009 IRS Form 990, which has some interesting tidbits an accountant may be able to dechiper.
I notice, for example, that NHF made a "gift" of $1,112,748 to the Seymour Diamond Fellowship Fund [of] the Diamond Headache Clinic Research and Education Foundation. Are the Diamonds using the NHF as their personal piggy bank?
Also, NHF paid $814,955 to Vedanta Associates Inc., an independent contractor, for "research on various projects and programs." Seems like a lot of money for "research." What I've been able to find out about Vedanta Associates is it "provides marketing research and medical communications solutions to the pharmaceutical and heathcare industry."